Is Singapore “winning the depopulation race?” according to global mortality statistics?
This post on X (formerly Twitter) last week has garnered significant views and shares. It claims that Singapore has won the “depopulation race” – experiencing the most excess mortality globally as a result of the pandemic. According to further posts, this is part of a wider conspiracy to depopulate the world through vaccination. 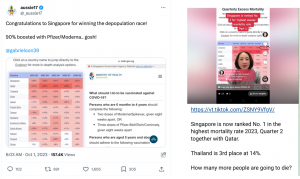 The post features a screenshot of a table that depicts Singapore at the top of a ranking of “excess mortality” and a second screenshot from the Ministry of Health (MOH) website about Covid-19 vaccination; implying that the two are linked.
The post features a screenshot of a table that depicts Singapore at the top of a ranking of “excess mortality” and a second screenshot from the Ministry of Health (MOH) website about Covid-19 vaccination; implying that the two are linked.
While the post does not provide a link to table of countries, we found the table on the online platform “Mortality Watch,” which describes itself as a “the world’s largest mortality data repository” and claims to also have the “most detailed” dataset on the internet.
While the platform does not display any affiliations at first glance, a closer look at the linked information on their “about” page redirects to a Substack page which focuses on vaccines and compiles research that, they suggest, disproves vaccine efficacy. The most recent post, which is based on data from Mortality Watch, concludes that “vaccines have clearly not ended the excess deaths and their correlation to the peaks of excess deaths is striking.”
Excess Mortality Data
To fact-check this claim, we first took a closer look at the data itself. According to Mortality Watch, “quarterly excess mortality” is derived from the crude mortality rate in all available countries. Clicking on the “2023 Q2” tab produces the same table from the screenshot in the claim.

“Excess mortality” is the difference between actual mortality (number of deaths from all causes) and expected mortality (projected based on historical data). According to the table above, in Quarter 2 of 2023 Singapore’s crude excess mortality was 37% more than the projected baseline for that specific quarter. Estimates of excess deaths can offer a look at overall mortality changes during the pandemic – not only from recorded Covid deaths, but from a range of factors such as indirect effects of the pandemic. However, it is vital to note that excess mortality is neither clear cut nor simple to calculate and compare.
Estimates of excess deaths can offer a look at overall mortality changes during the pandemic – not only from recorded Covid deaths, but from a range of factors such as indirect effects of the pandemic. However, it is vital to note that excess mortality is neither clear cut nor simple to calculate and compare.
Firstly, crude mortality rates (used by Mortality Watch) do not take into account the change in a population’s age structure over the past years. While crude rates offer direct snapshot of a specific time period, mortality comparisons (whether between time periods or different populations) are typically more accurately derived using age-standardisation. In Singapore’s case, this would account for our aging population, which has steadily increased over the past few years.
The percentages presented in the Mortality Watch table as a country-based comparison are even less robust considering they are also not standardised according to population or region. Similar to age-standardisation, it is not statistically robust to compare the morality rates of countries with entirely different baselines and population compositions. Instead, most of the published research we can find that analyses multiple countries use a standardisation formula to derive more accurate, representative comparisons.
While the specific percentage of 37% for Q2 in Singapore is therefore not technically inaccurate, the presentation of the data as a ranking across countries is misleading.
Secondly, projected baselines of expected deaths vary from study to study and can impact the robustness of results if not specifically calibrated according to country-specific trends. As such, researchers have emphasised that excess mortality is an estimation rather than a certain statistic. Further, excess death estimates are reliant on countries having accurate and detailed records and systems to record deaths, population data, and historical mortality trends – without which global excess death comparisons become less viable.
Mortality Databases
While researching excess mortality studies we also observed that published work on the subject often cites and draws from existing mortality databases – none of which include Mortality Watch.
Instead, referenced databases include the Human Mortality Database, the World Mortality Dataset, alongside recent data from the World Health Organisation (WHO) and the Economist among others. These databases are accompanied by detailed methodology explanations (much more than Mortality Watch provides), and as noted above, make use of more robust standardisations according to age and population rather than using crude rates. Even then, estimated rates vary between these databases due to different methodologies and research parameters.
Conclusion
This fact-check is not about finding the most accurate data or database or checking sources of each dataset. The key question is whether data from Mortality Watch accurately shows that Singapore has won the “depopulation race” and is ranked 1st in the world in excess mortality. Our research suggests that it does not.
Contrary to what the claim asserts, there isn’t a comprehensive global ranking of excess mortality rates. While excess deaths within Singapore are an ongoing subject of study and analysis and have undeniably been impacted by the pandemic, Singapore has not “won the depopulation race.” We give this claim a rating of False.
Can vaccines be linked to population changes in Singapore?
Beyond (incorrectly) identifying the “top” countries in the “depopulation race” the same user on X goes on to suggest a correlation between countries with higher vaccination levels and the top spots, and poorer countries occupying the lower spots because they “can’t afford the vax.” However, a look at vaccination statistics quickly reveals a false correlation. Some of the countries listed at the bottom spots according to this ranking of excess crude deaths such as Cyprus (which is almost at the bottom) and Greenland have relatively robust vaccination numbers – 54% and 68% respectively being fully vaccinated – moreso than some of the countries with higher excess deaths as presented by the Mortality Watch table.
However, a look at vaccination statistics quickly reveals a false correlation. Some of the countries listed at the bottom spots according to this ranking of excess crude deaths such as Cyprus (which is almost at the bottom) and Greenland have relatively robust vaccination numbers – 54% and 68% respectively being fully vaccinated – moreso than some of the countries with higher excess deaths as presented by the Mortality Watch table.
Another example of the unsupported correlation is how some countries with high vaccination numbers – similar to those of Japan and Thailand – such as Iceland had much lower excess deaths on the same Mortality Watch heatmap. Attempts to link vaccinations to excess deaths based on the Mortality Watch data are, therefore, demonstrably inaccurate. Replies to the original claim post have also included separate claims about Singapore in particular. One post claimed that Singapore has experienced the “highest number of perinatal deaths in 20 years,” as an additional sign of vaccine-caused harm.
Replies to the original claim post have also included separate claims about Singapore in particular. One post claimed that Singapore has experienced the “highest number of perinatal deaths in 20 years,” as an additional sign of vaccine-caused harm. 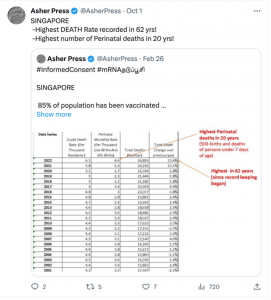
This claim was first made on social media in February this year, purporting that Singapore in 2022 had an increase in perinatal deaths and stillbirths of 50% to 70% – as seen in Singapore’s own official records.
However, despite users such as Aussie17 (the originator of the recent excess deaths post) sharing these statistics widely, it was later revealed that the jump in numbers was the result of Singapore broadening the official definition of stillbirths, which resulted in more being recorded for the year 2022. As “perinatal deaths” include stillbirths and infant death up to 7 days, the total perinatal death numbers also saw a similar increase in 2022. While Aussie17 issued a correction on their substack page, the original posts and other similar posts repeating the incorrect statistics remain on X with no correction and, as we can now observe, are repeated months later as fact.
Data and Accuracy
Although there is no mention of “depopulation” or vaccines as the cause of excess deaths on the Mortality Watch website, it stands out to us as lacking a stated purpose beyond existing to allow the generation of mortality charts. While other open-source platforms such as Our World in Data have stated objectives such as making progress against “the world’s largest problems,” Mortality Watch does not.
This becomes significant considering that accurate and robust data is collected not merely for the sake of compiling numbers and generating percentages. In the case of excess mortality, research objectives are often clearly stated – for instance to assess and improve healthcare or policy approaches, to identify vulnerable populations, or to gain a better understanding of key issues. These objectives are also typically reflected and described in their methodologies.
Our research on Mortality Watch suggests a lack of full transparency when it comes to how and why they are presenting their data. Coupled with the sparse methodology descriptions and their data only being referenced by claims relating to anti-vaccine theories (such as “depopulation theory”), caution is required when approaching claims based solely on their data. Cross-checking with other available research is key to reaching an informed perspective – particular with shocking claims such as this one.